




“I am so grateful that I have gotten to put my professional knowledge to use in order to help people during these unprecedented pandemic times,” said Natalie Crise (BS ’17, MS ’19). A graduate of The University of Tulsa’s bachelor’s and master’s programs in speech-language pathology, Crise today works for Tulsa’s Saint Francis Health System.

Many people likely have an idea that speech-language pathologists (SLPs) primarily work to help children overcome lisps and stutters or elderly people deal with cognitive deficits impacting their ability to communicate and complete daily tasks/activities. While many perform such roles, the COVID-19 pandemic has revealed a markedly different side of the profession, particularly for SLPs, such as Crise, who work in hospitals. Indeed, for the past 20 years, TU SLP alumna Teresa Bierig (BS ’92, MS ’94) has focused her career on the hospital setting, both in patient care and management roles. Today, she is deploying her specialized skills and knowledge to help COVID-19 patients at Tulsa’s Hillcrest Medical Center.
“SLPs working in hospitals during the COVID-19 pandemic have been on the frontlines of patient care,” Bierig noted. “We have all seen the devastation this virus can have on people, both patients and their loved ones.”
Swallowing
One of the main reason SLPs are an essential part of so many COVID-19 patients’ interdisciplinary care teams – including dietitians, respiratory therapists, nurses, physical and occupational therapists – is because of the swallowing deficits caused from being on a ventilator. These life-support machines mechanically pump oxygen into a critically ill person via a tube inserted down the throat and into the airway/lungs.

The throat, however, contains many important swallowing structures and it is easy to damage them when inserting and extracting a ventilator tube. As Bierig observed, “the breathing tube is a good thing in that it helps the patient to breathe; however, it is also a foreign object and can irritate the swallow mechanism’s tissues and muscles.” Added to such damage is the fact that a patient is physically unable to swallow while the ventilator tube is in place, thus progressively weakening the swallow mechanism and its associated muscles through inactivity.
Crise explained this complex situation and the dangers it poses: “The main structures and muscles work together to close of the airway and propel food and liquids down into the esophagus. But when the swallow structures are damaged or weakened, they can’t do their job to protect the airway. In that case, when a patient swallows, food and liquids travel down into the lungs. Over time, this can lead to aspiration pneumonia and worsen the respiratory issues that many COVID-19 patients are already facing.” Aspiration pneumonia also usually prolongs a person’s hospital stay.
Once a patient comes off a ventilator, the first thing a SLP does is assess any weakness or damage that may be present. The next step is to make recommendations to help the individual eat and drink safely, including modifying their diet, as well as teach them how to exercise and, thereby, strengthen their swallow mechanisms. For critically ill COVID-19 patients, noted Bierig, SLPs also focus on respiratory muscle strength-training. “This helps them to produce a cough that is sufficiently strong to cough out food, liquid and anything else that might have slipped into the airway.”
Speaking
Known in health care as “dysphagia,” difficulties swallowing are only one of the ventilator-related ailments with which SLPs help COVID-19 patients. Ventilator tubes can also cause trauma to a person’s delicate vocal cords. When a person is already physically weakened and perhaps even temporarily cognitively diminished from battling the coronavirus, a damaged larynx makes speaking all the more difficult.
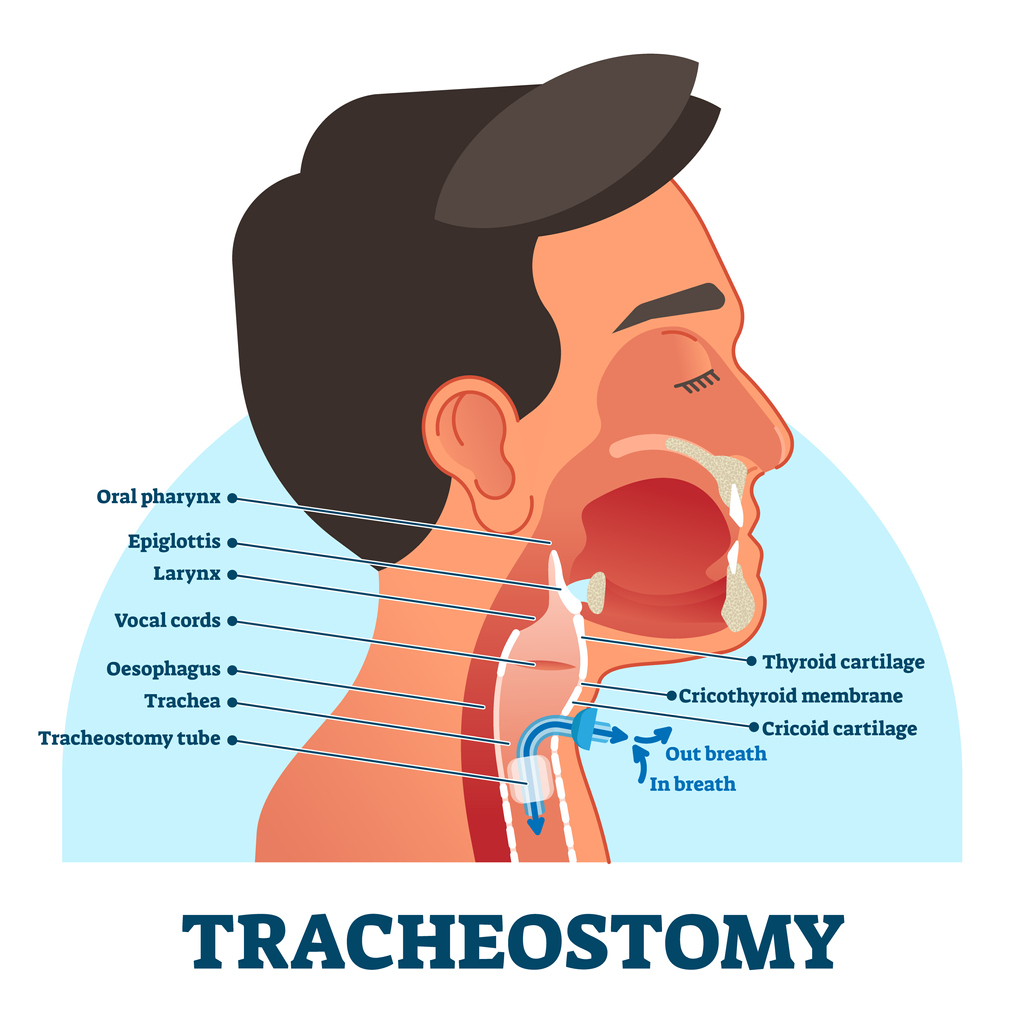 In addition, patients with severe cases of COVID-19 will often require insertion of a tracheostomy tube, which is inserted through a hole made in the front of the neck into the windpipe (trachea), in order to breathe. Patients commonly require tracheostomy tubes when they have been on a ventilator a long time and yet still cannot breathe on their own.
In addition, patients with severe cases of COVID-19 will often require insertion of a tracheostomy tube, which is inserted through a hole made in the front of the neck into the windpipe (trachea), in order to breathe. Patients commonly require tracheostomy tubes when they have been on a ventilator a long time and yet still cannot breathe on their own.
“When a patient has a tracheostomy tube in place,” explained Crise, “air from their lungs goes directly in and out from their neck, rather than passing through their vocal cords. Essentially, therefore, a person in that situation loses their voice.” Fortunately, there is a prosthetic device that can be fastened to the end of a tracheostomy tube that, by directing air back through the vocal cords, “gives them their voice back.”
Both Crise and Bierig have deployed these devices with numerous COVID-19 patients. One patient Crise recalled who found himself in this situation had contracted the virus in late December, was immediately placed on a ventilator and eventually switched to a tracheostomy tube. During all that time, he had been unable to utter a word to his loved ones. Crise saw him around the end of February, at which time she placed a speaking device on the end of his tube. “For the first time in two months he was able to talk,” Crise said. “We Facetimed all of his family members and they were so happy to finally hear his voice after such a long time. I went home after work that day feeling on top of the world.”
TU’s Department of Communication Sciences and Disorders offers undergraduate and master’s level education for prospective speech-language pathologists. Learn more about how to gain the knowledge and skills required to enter this in-demand health care profession.